Abstract
Peptide-based cancer vaccines represent a promising avenue in immunotherapy, leveraging the specificity of tumor-associated antigens (TAAs) to elicit targeted immune responses. Recent advancements have significantly enhanced the efficacy and applicability of these vaccines. The integration of artificial intelligence (AI) and other modern innovations has revolutionized the identification and optimization of epitopes,and is used for giving personalized medicine. AI models have demonstrated unprecedented accuracy in predicting peptide-MHC interactions, used for development of more effective vaccines.
The peptide vaccines have shown potential in various cancers, like breast, melanoma. For instance, personalized neoantigen vaccines have achieved promising results in early-phase trials, with some patients exhibiting durable responses. Additionally, off-the-shelf vaccines targeting common mutations, such as the KRAS mutation prevalent in pancreatic and colorectal cancers, have shown efficacy in preventing cancer recurrence. Despite these advancements, challenges remain, including issues related to low immunogenicity, HLA restriction, and the need for effective delivery systems. The convergence of AI, personalized medicine, and innovative vaccine platforms holds the promise of transforming peptide-based cancer vaccines into a cornerstone of cancer immunotherapy
Introduction
Cancer remains a leading cause of morbidity and mortality worldwide, there are many therapies associated with limited specificity and significant side effects. Peptide-based cancer vaccines have emerged as a promising immunotherapeutic strategy, leveraging the specificity of tumor-associated antigens (TAAs) to elicit targeted immune responses. These vaccines utilize short synthetic peptides representing specific TAAs for triggering the immune system, particularly cytotoxic T lymphocytes (CTLs), to recognize and eliminate cancer cells.
Recent advancements have significantly enhanced the efficacy and applicability of peptide-based vaccines. The integration of artificial intelligence (AI) has revolutionized the identification and optimization of epitopes, enabling the design of personalized vaccines tailored to individual tumor profiles. AI models like MUNIS and GraphBepi have accuracy in predicting peptide-MHC interactions, facilitating the development of more effective vaccines. Nature. Despite these advancements, challenges remain, including issues related to low immunogenicity, HLA restriction, and the need for effective delivery systems. However, ongoing research into novel adjuvants, delivery platforms, and combination therapies continues to address these limitations. The convergence of AI, personalized medicine, and innovative vaccine platforms holds the promise of transforming peptide-based cancer vaccines into a cancer immunotherapy
What is a Peptide Vaccine?
A peptide-based cancer vaccine is a therapeutic vaccine that uses short synthetic fragments of tumor proteins (peptides) to stimulate the immune system. These peptides are derived from tumor-associated antigens (TAAs) or tumor-specific antigens (TSAs) and are used to activate cytotoxic T lymphocytes (CTLs) and helper T cells. The immune system, once after the formation of memory of that antigen, can specifically recognize and destroy cancer cells expressing the targeted antigen, providing precision immunotherapy with minimal side effects (Liu et al., 2024; Kumar et al., 2024).
Types of Peptide-Based Vaccines
The peptide Based Vaccine are Classified Based on antigen selection and design.
1.Tumor-Associated Antigen (TAA) Peptide Vaccines
Derived from proteins overexpressed in cancer cells but also present in normal cells at low levels.
Example: HER2/neu-derived peptides in breast cancer (NeuVax).
2. Tumor-Specific Antigen (TSA) or Neoantigen Peptide Vaccines
Derived from mutations unique to tumor cells, not present in normal cells.
Highly personalized and immunogenic.
Example: EGFRvIII-targeted peptide vaccine in glioblastoma (Rindopepimut).
3.Synthetic Long Peptides (SLPs)
Longer peptides (20–35 amino acids) that contain multiple epitopes.
Enhance both CD4⁺ and CD8⁺ T cell responses.
4.Multi-Epitope Peptide Vaccines
Combine several epitopes in a single vaccine to target multiple antigens simultaneously.
Useful for heterogeneous tumors.
5.Personalized Neoantigen Vaccines
Custom-designed using patient-specific tumor genomics.
AI-guided prediction identifies high-affinity MHC-binding peptides for individual patients
Synthesis of Peptide-Based Cancer Vaccines
1. Epitope Identification and Selection
Tumor Antigens: Peptides are derived from tumor-associated antigens (TAAs) or tumor-specific antigens (TSAs) that are overexpressed or mutated in cancer cells.
Prediction Tools: Bioinformatics tools, such as NetMHCpan and TripHLApan, predict peptide-MHC binding affinities to identify potential epitopes arXiv.
2. Peptide Synthesis
Solid-Phase Peptide Synthesis (SPPS): The most common method, SPPS involves sequential addition of protected amino acids to a solid resin support. Each amino acid is coupled to the growing chain, followed by deprotection steps to remove protective groups, allowing the next amino acid to bind.
Microwave-Assisted Peptide Synthesis: This technique accelerates the coupling reactions by using microwave energy, leading to faster synthesis times and potentially higher yields.
Chemical Ligation Methods: For longer peptides or proteins, methods like native chemical ligation (NCL) can be employed. NCL involves the covalent joining of two unprotected peptide segments through a thiol exchange reaction, facilitating the synthesis of larger, more complex peptides.
3. Purification and Characterization
Purification: After synthesis, peptides are typically purified using high-performance liquid chromatography (HPLC) to remove any truncated sequences or impurities.
Characterization: Techniques such as mass spectrometry and analytical HPLC are used to confirm the identity and purity of the synthesized peptides.
4. Conjugation to Delivery Systems
Adjuvants: Peptides are often conjugated to adjuvants to enhance their immunogenicity. Common adjuvants include aluminum salts, emulsions, and Toll-like receptor (TLR) agonists.
Carrier Proteins: To improve the uptake and presentation of the peptide, they can be conjugated to carrier proteins like keyhole limpet hemocyanin (KLH) or diphtheria toxoid.
Nanoparticles: Encapsulation in nanoparticles, such as liposomes or lipid nanoparticles, can protect peptides from degradation and facilitate targeted delivery to antigen-presenting cells.
5. Formulation and Administration
Formulation: Peptide vaccines are formulated into suitable forms for administration, such as injectable solutions or lyophilized powders.
Administration Routes: Common routes include subcutaneous, intramuscular, or intradermal injections. The choice of route can influence the type of immune response elicited.
Mechanism of Action of Peptide-Based Cancer Vaccines
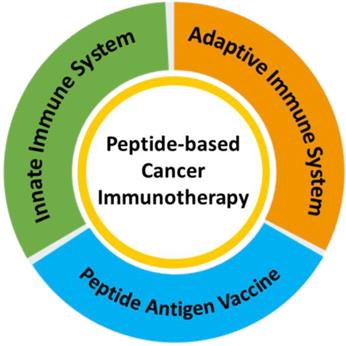
Peptide-based cancer vaccines are designed to elicit specific adaptive immune responses against tumor-associated antigens (TAAs) or tumor-specific neoantigens (TSAs). Their mechanism involves antigen presentation, T cell activation, and targeted tumor cell killing.
- Antigen Uptake and Processing
Peptide Delivery:
Synthetic peptides are delivered via injection (subcutaneous, intradermal, or intramuscular), often combined with adjuvants or nanoparticle carriers to enhance uptake.
Internalization by Antigen-Presenting Cells (APCs):
Peptides are captured by dendritic cells (DCs), macrophages, or Langerhans cells in the skin and lymphoid tissues (Kumar et al., 2024).
Proteolytic Processing:
Short peptides are directly loaded onto MHC class I molecules, while longer peptides are processed into smaller epitopes in the endosome for MHC class II presentation.
- Antigen Presentation
MHC Class I Pathway:
Peptides presented on MHC I molecules activate CD8⁺ cytotoxic T lymphocytes (CTLs).
CTLs recognize and destroy tumor cells expressing the target antigen (Liu et al., 2024).
MHC Class II Pathway: Peptides presented on MHC II molecules activate CD4⁺ helper T cells, which secrete cytokines to enhance CTL and B cell responses.
- T Cell Activation
Signal 1 – TCR Recognition:
The T cell receptor (TCR) binds to the peptide-MHC complex on APCs.
Signal 2 – Co-stimulation:
Co-stimulatory molecules (e.g., CD80/CD86 on APCs interacting with CD28 on T cells) provide essential activation signals.
Signal 3 – Cytokine Signaling:
APCs release cytokines (IL-12, IFN-γ) to polarize T cells towards a Th1 cytotoxic response.
- Immune Effector Function
CD8⁺ Cytotoxic T Cells:
Activated CTLs migrate to the tumor site and recognize antigen-expressing tumor cells.
They induce apoptosis via performing/granzyme pathways or Fas-FasL signaling.
CD4⁺ Helper T Cells:
Provide cytokine support, enhance CTL activity, and stimulate B cell-mediated antibody production against tumor antigens.
Memory Formation:
Some activated T cells differentiate into memory T cells, ensuring long-term immune surveillance against tumor recurrence (Skwarczynski & Toth, 2015).
- Enhancement by Modern Innovations
Adjuvants:
Toll-like receptor (TLR) agonists or saponins enhance DC maturation and cytokine production.
Nanoparticles and Delivery Systems:
Improve peptide stability, facilitate targeted delivery, and enhance antigen presentation to APCs (Falcone et al., 2025).
Neoantigen Personalization:
AI-guided epitope prediction ensures the peptide sequences elicit strong and patient-specific immune responses (Nature Communications, 2025)
Clinical Applications of Peptide-Based Cancer Vaccines
Peptide-based cancer vaccines have shown promise in various clinical settings, particularly in cancers with well-characterized tumor-associated antigens (TAAs) and tumor-specific antigens (TSAs). These vaccines aim to stimulate the immune system to recognize and eliminate cancer cells expressing specific antigens.
1. HER2-Positive Breast Cancer
Vaccine: HER2-ICD vaccine
Clinical Trial: A Phase I trial demonstrated that this vaccine was safe and generated robust, long-lasting T and B cell immune responses in patients with HER2-positive breast cancer. Notably, 75–85% of patients remained alive 10 years post-vaccination, with half experiencing no recurrence ASCOPubs.
2. Melanoma
Vaccine: Personalized Neo-Antigen Peptide Vaccine (PNV21-001)
Clinical Trial: A Phase I study assessed the safety of this vaccine in patients with stage IIIC–IV melanoma or hormone receptor-positive, HER2-negative metastatic refractory breast cancer. The vaccine, combined with the Th1-polarizing adjuvant poly ICLC, induced polyclonal, poly-epitope, cytolytic T cell immunity against the patient’s tumor Fred Hutch.
3. Pancreatic and Colorectal Cancer
Vaccine: KRAS-targeted peptide vaccine
Clinical Trial: A Phase I trial involving 25 patients with pancreatic or colorectal cancer harboring specific KRAS mutations demonstrated that the vaccine is safe and stimulates the patient’s immune system to create cancer-fighting cells. This approach is particularly relevant as about 90–95% of pancreatic cancer and 50% of colon cancer cases have a KRAS mutation Memorial Sloan Kettering Cancer Center.
4. Hepatocellular Carcinoma (Liver Cancer)
Vaccine: Personalized peptide vaccine combined with immunotherapy
Clinical Trial: A small, early trial by U.S. researchers found that this personalized vaccine, when combined with the immunotherapy drug Keytruda, led to significant tumor shrinkage in nearly a third of patients with advanced liver cancer. This effect is about twice the typical response rate seen with immunotherapy alone Reuters.
5. Ovarian Cancer
Vaccine: Peptide-based vaccine targeting specific antigens
Clinical Application: Research has shown that peptide vaccines can be effective in treating ovarian cancer by targeting specific tumor antigens. These vaccines aim to stimulate the immune system to recognize and eliminate cancer cells, offering a promising therapeutic strategy
AI-Driven Approaches in Peptide-Based Cancer Vaccine Development
Artificial Intelligence (AI) is revolutionizing peptide-based cancer vaccines by enhancing precision, personalization, and speed throughout the vaccine development process. AI integrates machine learning (ML), deep learning (DL), and bioinformatics tools to optimize epitope selection, vaccine design, and immune response prediction.
- Epitope and Neoantigen Prediction
AI algorithms analyze tumor genomic and proteomic data to identify tumor-specific antigens (TSAs) and neoantigens with high immunogenicity.
Models like MUNIS, NetMHCpan, GraphBepi, and DeepVacPred predict peptide-MHC binding affinity, ensuring that selected peptides elicit strong T cell responses (nature.com, 2025).
AI helps prioritize high-affinity epitopes for personalized vaccines, minimizing off-target effects and enhancing safety.
- Personalized Vaccine Design
AI integrates patient-specific genomic, transcriptomic, and immunopeptidomic data to design custom peptide vaccines.
Enables tailoring vaccines to individual tumor mutations, improving efficacy and reducing immune evasion.
Facilitates the design of multi-epitope or long-peptide vaccines targeting multiple tumor antigens simultaneously (Ludwig Cancer Research, 2025).
- Vaccine Construct Optimization
AI predicts codon usage, secondary mRNA structures, and untranslated regions (UTRs) for mRNA/peptide vaccines, enhancing stability, translation efficiency, and immunogenicity (mdpi.com, 2025).
Machine learning models help design optimal adjuvant combinations and delivery platforms for enhanced antigen presentation.
- Immune Response Simulation
AI models simulate the immune system’s response to candidate peptides using silico immune modeling.
Predicts T cell and B cell activation, cytokine release, and potential tumor escape mechanisms.
Reduces time and cost by filtering less effective candidates before in vitro/in vivo testing.
- Accelerated Clinical Trial Design
AI assists in patient stratification, biomarker identification, and dose optimization, improving trial efficiency.
Predicts which patients are most likely to respond to a vaccine, reducing trial failures and expediting regulatory approval (investors.com, 2024).
- Integration with Modern Delivery Systems
AI guides the design of nanoparticle, hydrogel, or microneedle delivery systems, optimizing peptide stability and controlled release.
Ensures effective antigen presentation to dendritic cells (APCs), maximizing T cell activation (News-Medical.net, 2025).
Collaborations and Research Networks
1. Academia-Industry Partnerships
Universities collaborate with biotech and pharmaceutical companies to translate peptide vaccine research into clinical trials.
Example: BioNTech, Moderna, and CureVac are developing peptide or mRNA-based cancer vaccines incorporating tumor-specific antigens.
2. International Research Consortia
Cancer Vaccine Consortia focus on:
Epitope discovery,Vaccine formulation optimization,Multi-center clinical trials for various cancers
Collaborative platforms ensure standardization, data sharing, and rapid innovation
- AI and Computational Collaborations
Partnerships with AI-driven biotech firms help in:Neoantigen prediction,Immune response modeling,Personalized vaccine design
This accelerates the transition from bench to bedside, ensuring vaccines are tailored to individual patient tumors.
4. Clinical Trial Networks
Peptide vaccines are evaluated through Phase I–III clinical trials, often in multi-center global collaborations, to assess:Safety,Immunogenicity
,Clinical efficacy
Collaboration ensures large patient cohorts, increasing statistical significance and accelerating regulatory approval.
Challenges of Peptide-Based Cancer Vaccines
Despite their promising potential, peptide-based cancer vaccines face several challenges that limit their clinical efficacy. These challenges include biological, technological, and clinical barriers:
- Low Immunogenicity
Short peptides often fail to elicit a strong immune response without adjuvants or delivery systems.Poor uptake by antigen-presenting cells (APCs) can result in suboptimal T cell activation.
Strategies like long peptides, multi-epitope constructs, and potent adjuvants are required to enhance immunogenicity (Skwarczynski & Toth, 2015).
- Peptide Stability and Degradation
Free peptides are prone to enzymatic degradation in vivo.
Rapid clearance reduces the duration of antigen presentation, limiting immune activation.Encapsulation in nanoparticles, liposomes, or hydrogels can improve stability (Hos et al., 2018).
- Tumor Heterogeneity and Immune Escape
Tumors often downregulate antigen expression or mutate target epitopes, allowing immune evasion.Single-peptide vaccines may fail due to antigen loss.
Multi-epitope or personalized vaccines are needed to address tumor heterogeneity (Kumar et al., 2024).
- MHC Restriction
Peptides must bind specific HLA alleles for effective T cell activation.
Population-level HLA diversity limits universality of peptide vaccines.
Computational prediction and personalized vaccine design using AI-based HLA typing can partially overcome this limitation (Nature Communications, 2025).
- Limited Efficacy as Monotherapy
Peptide vaccines alone often produce modest clinical responses, particularly in immunosuppressive tumor microenvironments.
Combination with checkpoint inhibitors, cytokines, or chemotherapy is usually necessary to achieve significant anti-tumor effects (Liu et al., 2024).
- Manufacturing and Scalability Challenges
Personalized vaccines require patient-specific sequencing and peptide synthesis, increasing time and cost.
Large-scale clinical application may be limited by manufacturing complexity and quality control.
- Regulatory and Clinical Trial Barriers
Novel peptide constructs, delivery systems, and AI-based designs require rigorous clinical testing.
Regulatory approval is complex due to individualized therapy approaches
Future Prospects
The integration of AI into peptide-based cancer vaccine development holds promise for:
Enhanced Precision: AI enables the design of vaccines tailored to individual tumor profiles, improving treatment outcomes.
Accelerated Development: AI streamlines the vaccine development process, reducing time from concept to clinical application.
Improved Efficacy: AI-driven optimization of vaccine constructs and delivery systems enhances immune responses
Advantages of Peptide-Based Cancer Vaccines
Peptide-based cancer vaccines are emerging as a promising immunotherapy approach due to their ability to specifically target tumor antigens while offering a favorable safety and efficacy profile. Compared to conventional therapies, they provide precision, personalization, and versatility.
- High Specificity for Tumor Cells
Peptide vaccines are designed to mimic tumor-associated antigens (TAAs) or tumor-specific neoantigens (TSAs).
This allows activation of cytotoxic CD8⁺ T cells that selectively attack tumor cells expressing the target antigen, minimizing damage to healthy tissues.
Reduces off-target effects seen with chemotherapy or non-specific immunotherapies (Skwarczynski & Toth, 2015).
- Safety and Minimal Toxicity
Being synthetic and non-replicating, peptide vaccines do not carry risks of infection.
Do not induce systemic toxicity or autoimmune reactions when appropriately designed.
Can be combined with immune checkpoint inhibitors without significantly increasing adverse effects (Liu et al., 2024).
- Ease of Synthesis and Customization
Solid-phase peptide synthesis (SPPS) allows rapid and reproducible production of peptides.
High-throughput platforms enable production of multiple peptides simultaneously, facilitating multi-epitope or personalized vaccine formulations.
Cost-effective and scalable for clinical production (Kalita & Saha, 2022).
- Personalized Immunotherapy
Integration with next-generation sequencing (NGS) and AI-driven neoantigen prediction allows identification of patient-specific tumor antigens.
Personalized vaccines enhance immunogenicity and reduce the risk of immune evasion by tumors.
Supports precision medicine approaches, increasing therapy success (Nature Communications, 2025).
- Induction of Robust Immune Responses
Peptide vaccines can stimulate CD8⁺ cytotoxic T lymphocytes (CTLs) for tumor killing and CD4⁺ helper T cells for cytokine support.
With appropriate adjuvants, vaccines can induce long-lasting memory T cells, providing durable protection and reducing tumor relapse (Kumar et al., 2024).
- Versatility and Compatibility with Combination Therapies
Can be combined with checkpoint inhibitors (anti-PD-1, anti-CTLA-4), cytokines, or chemotherapy to enhance antitumor efficacy.
Synergistic effects improve tumor clearance, immune memory, and overall survival in preclinical and clinical studies.
Conclusion
Peptide-based cancer vaccines have emerged as a highly specific and safe therapeutic approach, leveraging tumor-associated antigens (TAAs) and tumor-specific neoantigens (TSAs) to activate cytotoxic T lymphocytes and helper T cells. They offer significant advantages over conventional therapies, including minimal toxicity, targeted immune activation, and the potential for long-term immune memory.
Recent innovations in vaccine delivery systems, such as lipid nanoparticles, lipopeptide hydrogels, and microneedle patches, have enhanced peptide stability, antigen presentation, and immune response. Furthermore, the integration of artificial intelligence (AI) and bioinformatics has revolutionized epitope prediction and personalized vaccine design, enabling the creation of patient-specific vaccines with optimized immunogenicity (nature.com, 2025; Falcone et al., 2025).
Clinical studies in breast cancer, melanoma, pancreatic cancer, liver cancer, and glioblastoma demonstrate that peptide vaccines are not only safe but also capable of generating robust and durable antitumor immune responses. Personalized neoantigen vaccines, in particular, have shown promising efficacy in early-phase trials, highlighting the potential of precision immunotherapy in oncology (Fred Hutch, 2024).
In conclusion, peptide-based cancer vaccines, supported by modern technological and AI innovations, represent a promising frontier in cancer treatment, bridging the gap between personalized medicine and immunotherapy, and offering hope for improved patient outcomes in multiple cancer types.
Reference
Liu, D., Wang, X., & Li, J. (2024). Peptide-Based Cancer Vaccines: Current Status and Future Directions. Vaccines, 12(8), 950. https://www.mdpi.com/2076-393X/12/8/950
Nature Communications. (2025). AI-Powered Neoantigen Prediction for Personalized Cancer Vaccines. https://www.nature.com/articles/s41541-025-01258-y
Falcone, N. (2025). New Delivery System Could Improve the Effectiveness of Peptide-Based Cancer Vaccines. News-Medical.net. https://www.news-medical.net/news/20250128/New-delivery-system-could-improve-the-effectiveness-of-peptide-based-cancer-vaccines.aspx
Fred Hutchinson Cancer Center. (2024). Personalized Neo-Antigen Peptide Vaccine for Melanoma and Metastatic Breast Cancer. https://www.fredhutch.org/en/research/clinical-trials/trial-details.fh_trial_id_14207.personalized-neo-antigen-peptide-vaccine-for-the-treatment-of-stage-iiic-iv-melanoma-or-hormone-receptor-positive-her2-negative-metastatic-refractory.html
ASCO Journals. (2024). HER2-Targeted Peptide Vaccine for Breast Cancer: Phase I Clinical Trial Results. https://ascopubs.org/doi/10.1200/JCO.2024.42.16_suppl.550
Reuters. (2024). Personalized Peptide Vaccine Shrinks Liver Tumors in Small Trial. https://www.reuters.com/business/healthcare-pharmaceuticals/geneos-cancer-vaccine-shrinks-liver-tumors-small-trial-2024-04-07/
Axios. (2025). KRAS-Targeted Peptide Vaccine Shows Promise in Pancreatic and Colorectal Cancer. https://www.axios.com/2025/08/14/vaccine-pancreatic-colorectal-cancer-study
MDPI. (2025). Advances in mRNA and Peptide Vaccine Development Using AI. https://www.mdpi.com/2673-6411/5/2/5
Ludwig Cancer Research. (2025). An AI-Powered Pipeline for Personalized Cancer Vaccines. https://www.ludwigcancerresearch.org/news-releases/an-ai-powered-pipeline-for-personalized-cancer-vaccines/
By
1] G.Pranav Karthick
kaniyakumari medical mission research center
2] V.S.Vishali Priya
Kanyakumari medical mission research center